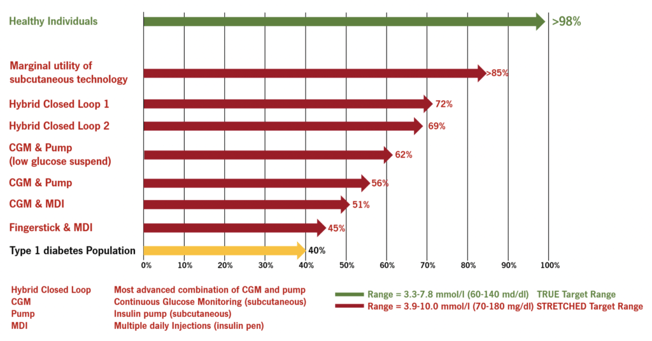
Figure 1: Overall, the “time in range” for patients with Type 1 diabetes is around 40% (yellow bar) and around 98% (green bar) for healthy people. By applying different technologies, the “time in range” can be increased to around 70% (red bars) under the ideal conditions of clinically controlled studies and the application of an increased upper limit of the target range (10.0 mmol/l = 180 mg/dl).
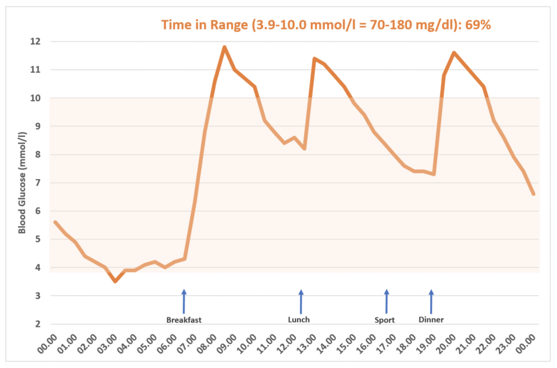
Figure 2: If the extended target range of 10.0 mmol/l (180 mg/dl) is applied to a blood sugar curve, a “time in range” of 69% results.
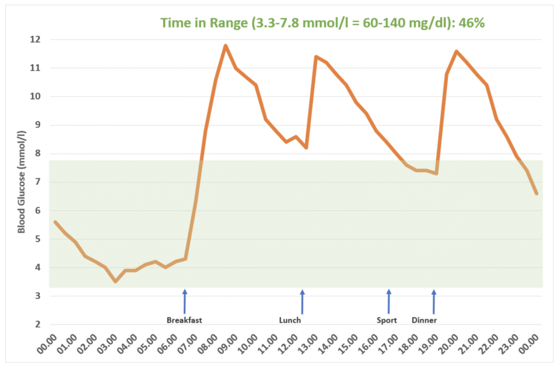
Figure 3: If the upper limit of the target range of 7.8 mmol/l (140 mg/dl), which also applies to healthy people, is applied to the same blood glucose curve, the “time in range” is reduced by about one third to 46%.
Under everyday conditions and using the narrower target range with an upper limit of 7.8 mmol/l (140 mg/dl), it can be assumed that the “time in range” achieved with these systems is more likely to be around 40 – 50% and the marginal benefit below 60% “time in range”. In any case, the room for improvement which Seraccess can implement in the blood based on glucose measurement in plasma or insulin dosage is considerable.
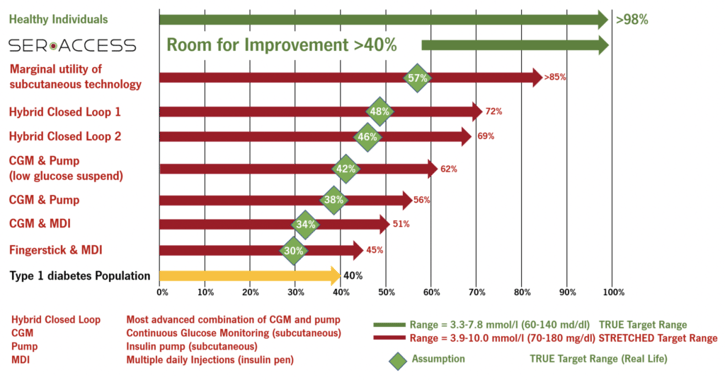
Figure 4: Overall, the “time in range” for patients with Type 1 diabetes is around 40% (yellow bar) and around 98% (green bar) for healthy people. By applying different technologies, the “time in range” can be increased to around 70% (red bars) under the ideal conditions of clinically controlled studies and the application of an increased upper limit of the target range (10.0 mmol/l = 180 mg/dl). Under everyday conditions and the application of an upper limit of the target range of 7.8 mmol/l (140 mg/dl), the “time in range” should be considerably lower (green squares), with the room for improvement correspondingly high and within the range of at least 40% (green arrow).
In the end, a constantly effective control of the blood sugar level leads to a higher “time in range”, which in turn leads to sustainably better blood sugar values and, consequently, to a reduction of acute (hypoglycaemia) and long-term complications (hyperglycaemia). It is therefore assumed that increasing the “time in range” by 10% leads to a reduction of the “long-term sugar” (HbA1c) by 0.5% – 0.8%, which in turn leads to a reduction of long-term complications by an additional 10% – 16%.(7-9)
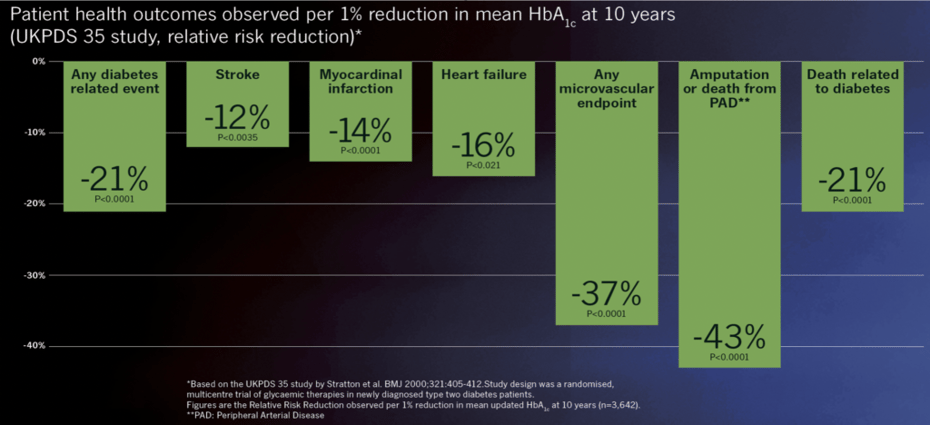
Figure 5: In the UKPDS 35 study, a 1% reduction in HbA1c over 10 years in newly diagnosed Type 2 diabetes patients significantly reduced the risk of diabetes-related sequelae, complications and deaths.
Conventional integrated systems (CGM with insulin pump) do not allow optimal control of blood sugar.
The preferred route to more effectively regulate blood sugar within the target area is to
- measure blood sugar directly in the blood without delay
- accurately and precisely measure blood sugar using the photometric method, and
- deliver insulin directly to the bloodstream so that it can deliver, without delay, its effect of lowering blood sugar
Since only the patented Seraccess technology communicates and interacts directly with the blood, it is the only one that has the potential to achieve this necessary and greatly improved blood glucose control in this way and, subsequently, to enable these patients to live a better life by preventing sequelae and complications
References
-
-
Freckmann et al. J Diabetes Sci Technol 2007;1(5):695-703
-
Medtronic Minimed 670G Pivotal Study JAMA. 2016;316(13):1407-1408
-
Weiss R. et al. ASPIRE Study Diabetes Technol Ther 2015 Aug 1; 17(8):542-547
-
Bergenstal R. et al. STAR-3 Study NEJM 2010;363:311-20
-
Ruedy K et al. DIAMOND Trial J Diabetes Sci Technol 2017;11(6):1138-1146
-
https://diatribe.org/time-range-whats-achievable-goal-diabete
https://diatribe.org/cgm-and-time-range-what-do-diabetes-experts-think-about-goals
last accessed 18.06.2019 -
The Diabetes Control and Complications Trial Research Group. The Absence of a Glycemic Threshold for the Development of Long-Term Complications: The Perspective of the Diabetes Control and Complications Trial. Diabetes 1996;45:1289-1298
-
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with cnventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet 1998; 352:837-853
-
American Diabetes Association. Eeg-Olofsson K, et al “HbA1c reduction and risk of cardiovascular diseases in type 2 diabetes: An observational study from the Swedish NDR”. ADA 2012
-